Stay informed on the COVID-19 scientific updates and other global health issues. Click here to sign up for email updates from ISGlobal.
After April 3rd, the day Caly et al. published their in vitro results about ivermectin and SARS-CoV-2, the research world and the general public was pulled into two extreme and opposite views about this topic. One group called for an early kill of the drug for its use against COVID-19, because the effective concentrations reported by Caly et al. were too high to be achieved in vivo and therefore any effort invested in pursuing this would be a waste and generate a false sense of hope. The other group, following a rightful sense of urgency, launched into promoting widespread use, even without appropriate evidence of efficacy and, more importantly, of safety for this specific use. Both extremes are equally wrong. Here we provide answers to common questions on this topic and show the involvement of ISGlobal researchers in finding answers to some of them.
What is ivermectin?
Ivermectin is an anti-parasitic drug developed during the 1970s as a partnership between the Kitasato Institute in Japan and Merck & Co. The project was led by Satoshi Omura and William Campbell on each side respectively. Given its broad spectrum against internal and external parasites that improved animal health and boosted productivity, ivermectin quickly became a blockbuster drug in the veterinary field.
During the 1970s, the world was waging a war against river blindness, also known as onchocerciasis, a disease caused by the Onchocerca volvulus parasite in rural areas that crippled whole communities. Some success had already been achieved thanks to the involvement of the World Bank. But once ivermectin was commercialized, it was noticed that Onchocerca cervicalis, the agent of onchocerciasis in horses, practically disappeared in areas where the new drug was used.

The burden of onchocerciasis: children leading blind adults in Africa.
[Image: Otis Historical Archives National Museum of Health & Medicine]
This lead to accelerated efforts to test ivermectin in humans that ended with the approval of the French regulatory authorities in the early 1980s and was followed by the unprecedented decision by Merck & Co. to donate as much ivermectin as needed, for as long as needed to eradicate river blindness. This gave birth to the Mectizan donation program. This program has distributed more than 3 billion treatments over the last 30 years and contributed to save countless lives throughout this period. The program was later expanded to include Lymphatic filariasis, another debilitating disease caused by filarial worms.

Elephantiasis of leg due to filariasis, in Luzon, Philippines. [Image: CDC]
Omura and Campbell were awarded the Nobel prize for physiology or medicine in 2015 for this discovery, an honour shared with Tu Youyou, the Chinese researcher responsible for the discovery of the antimalarial artemisinin.
More information on the story and the uses of ivermectin, here.
What is ivermectin used for in humans?
Here we describe some of the approved uses around the world.
1. In the US, ivermectin is marketed at doses of up to 200 mcg/kg once a year for the following indications:
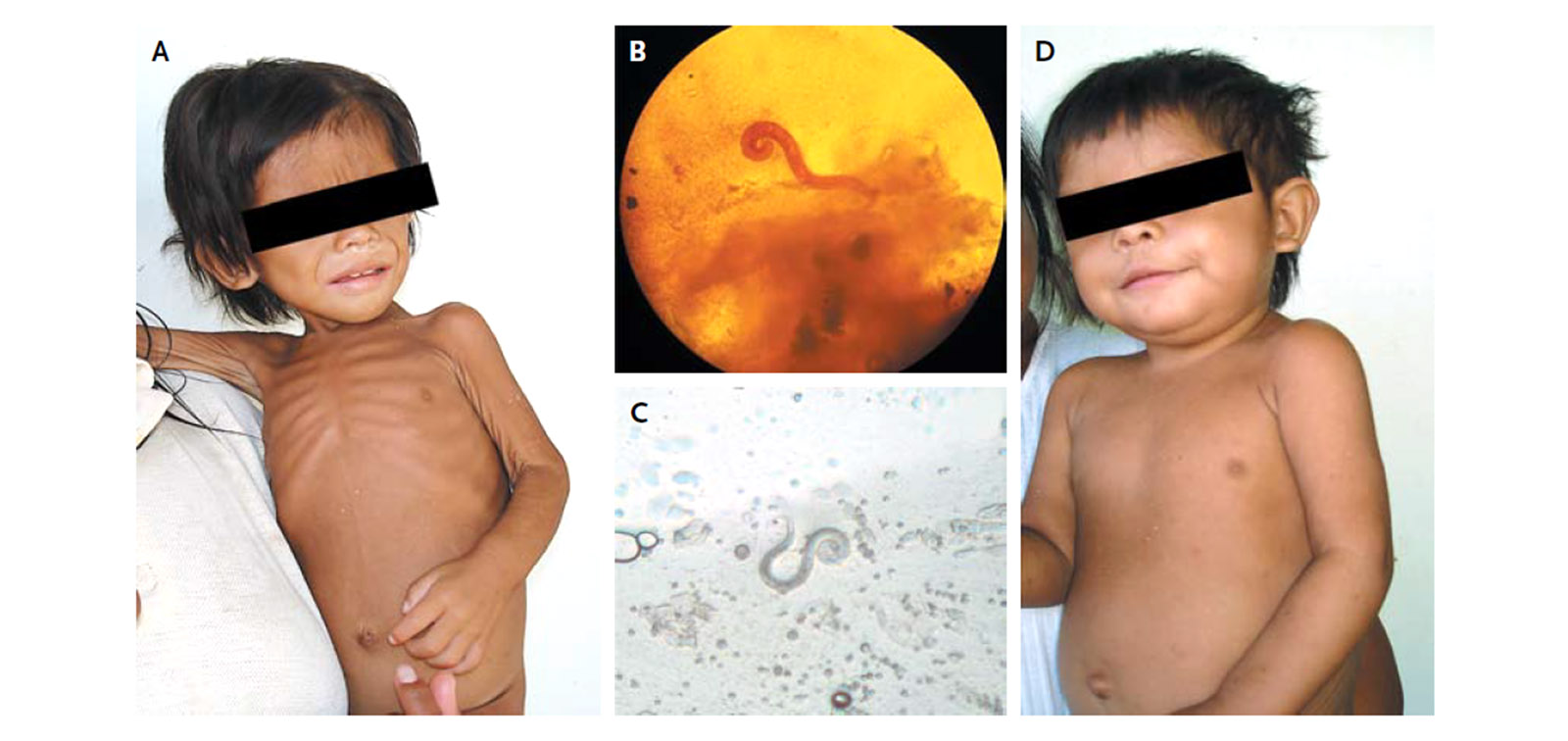
A two-year-old girl with disseminated strongyloidiasis cured with ivermectin (A) before, (B) faecal sample, (C) sputum sample and (D) six weeks after treatment. [Image from Chaccour and Del Pozo, NEJM, 2012]
- b. Onchocerciasis or river blindness
2. In Europe, ivermectin is also marketed against Lymphatic filariasis and scabies at single doses of up to 400 mcg/kg.
3. In Australia, 3 or more-200 mcg/kg doses within a month are recommended for the treatment of severe crusted scabies.
One promising line of work in which ISGlobal researchers have been deeply involved is the use of ivermectin at population level to kill mosquitoes and reduce malaria transmission
Any other proven or potential uses?
Although not marketed for these indications, ivermectin has partial efficacy against other common intestinal parasites in humans such as Ascaris lumbricoides and Trichuris trichura.
It is also sometimes used out of label against ectoparasites like head lice and Tunga penetrans among many other internal or external parasites.
One promising line of work in which ISGlobal researchers have been deeply involved is the use of ivermectin at population level to kill mosquitoes that feed on treated humans or animals and reduce malaria transmission.
Is ivermectin safe?
When used for the current indications, at the currently approved doses, ivermectin is a very safe drug. To date, more than three billion treatments have been distributed in the context of the Mectizan Donation Program alone with an excellent safety profile. Most adverse reactions are mild, transitory and associated with parasite death rather than with the drug itself.
Ivermectin targets the glutamate-gated chlorine channels that are only present in invertebrates. Mammals only express a similar channel that could cross react with ivermectin (the GABA-gated chlorine channels), but these are only expressed in the central nervous system and are protected by the blood brain barrier, a system of pumps that keeps potential toxics outside our nervous system. In spite of that, Rebecca Chandlerdescribed a series of 28 cases with severe neurological adverse reactions after ivermectin treatment outside onchocerciasis endemic areas.
When used for the current indications, at the currently approved doses, ivermectin is a very safe drug
In individuals infected with a high burden (>30.000 mf/ml) of the parasite known as Loa loa, ivermectin treatment can lead to severe encephalopathy and death. This has prevented the administration of ivermectin in several countries of central Africa, where the recent test-and-not-treat strategy may allow for the use of the drug.
There is no robust evidence to support the use of ivermectin in children under 15 kg of weight. There is no evidence to support the use of ivermectin during pregnancy.
Is ivermectin safe at higher doses than approved?
Guzzo et al. conducted a study with escalating doses of ivermectin in which some volunteers safely received doses of up to 2,000 mcg/kg, i.e. ten times the approved dose for onchocerciasis.
Although not described by Guzzo, persons receiving ivermectin at doses of 800 mcg/kg or above in other studies have sometimes described transient visual disturbances.
Smit et al. safely administered 600 mcg/kg daily for three days.
Does ivermectin have anti-viral properties?
Yes. Ivermectin has been proven to inhibit the replication of several RNA viruses such as:
Could ivermectin have a role in the treatment or prevention of COVID-19?
Perhaps, but the answer is not straightforward.
The in vitro experiments by Caly et al. were done by adding ivermectin into a cellular culture infected with the virus on a petri dish. The concentrations shown to reduce the viral replication by 50% and 99% in these experiments were 2.8 and 5 microMolar respectively.
To put this into perspective, the maximum concentration achieved in the blood after a single oral dose of 200 mcg/kg (the usual dose for river blindness) is of 40 ng/ml. 2.8 microMolar is the equivalent of 2,450 ng/ml, i.e. 60-fold higher than the maximum concentration after usual doses or 10-fold the maximum concentration observed in the high-dose Guzzo study.
Then why bother researching this?
COVID-19 is a public health emergency of international concern and there is no specific treatment for it. This fact, together with the excellent safety profile of ivermectin combine to warrant research on its potential use. Additionally, extrapolating directly from a Petri dish into a live organism is not correct. Several factors may contribute to make ivermectin efficacious in vivo at lower doses than those described by Caly et al, here are some of them:
Stay informed on the COVID-19 scientific updates and other global health issues. Click here to sign up for email updates from ISGlobal.
- Immune system. A cellular culture is just a layer of cells in a Petri dish and contains no immune system to combat the virus “side by side” with ivermectin.
- Viral load. The virus to cell ratio in a petri dish maybe way off what can be expected in an organism i.e. there may be an excess of virus-to-cells in the culture that would unbalance the fight in favour of the virus and make the in vitro results underestimate the true effect of ivermectin.
- Immunomodulatory effect. Ivermectin has the capacity to modulate the immune response. An exacerbated immune response is partly responsible for the pathophysiology of COVID-19.
- Previous in vitro - in vivo mismatch. Some in vivo effects may be possible even if efficacious in vitro concentrations are not attainable. A recent phase III clinical trial in dengue patients in Thailand, in which a once-daily dose of 400 μg/kg for three days was found to be safe but did not produce any clinical benefit, showed a modest and indirect in vivo effect against dengue, reducing the circulation of certain viral proteins.
- Was the right cellular line used? VERO cells are African green monkey kidney cells, although they are widely used in viral culture and in vitro experiments, they may not be the best platform for SARS-CoV-2. After showing promising results in VERO cells, hydroxychloroquine did not have the same effect in human lung cell cultures. In the case of ivermectin, this effect could either favour ivermectin or reduce its efficacy.
- Other potential mechanisms of action include inhibition of the viral enzyme used to unwind its RNA, the helicase, for which it seems ivermectin may be effective at much lower concentrations. Interaction with the Nicotinic Acetylcholine receptor that may cause immunomodulation or reduce the expression of ACE-II, the receptor used by the virus to enter the cells.
- What about the Importin alpha/beta? Importins are intracellular transport proteins sometimes used by viruses to enter the nucleus and replicate their genetic material. Ivermectin inhibits the importin and this has been amply quoted as the potential mechanism of action against SARS-CoV-2. This may have an effect on COVID-19 through a direct or indirect mechanism1.
In summary, there is equipoise. This is a term used in bioethics to define a situation in which there is reasonable doubt of whether a drug might be of use or not. Testing of ivermectin against SARS-CoV-2 in clinical trials is warranted.
Then why are we not giving ivermectin to those that need it today? People are dying!
The process for bringing a drug into widespread use is highly regulated. This is for good reasons. Lessons have been learned after some serious tragedies.
The main requisites for approving a drug to be used at population level is proven efficacy and safety. For ivermectin, there is robust evidence of safety when used for the approved indication at the approved doses. There is very limited evidence about the safety of ivermectin at higher doses (see table link above) and even less evidence for its safety when used in COVID-19 patients that tend to have proinflammatory states. These pro-inflammatory states may increase the penetration of ivermectin into the central nervous system with unknown consequences (see safety above). Other potential issues include drug-drug interactions with some antivirals given to COVID-19 patients such as ritonavir which may increase the levels of ivermectin.
Given the absence of reasonable evidence that ivermectin has any efficacy against SARS-CoV-2, the risk-benefit analysis dictates that we should be prudent
Given the absence of reasonable evidence that ivermectin has any efficacy against SARS-CoV-2, the risk-benefit analysis dictates that we should be prudent, i.e. evaluate the efficacy (and safety in this context) before taking ivermectin to the population level.
The evidence of efficacy should come from randomized, controlled (preferably double-blind) clinical trials which are studies in which patients are randomly allocated to receive ivermectin or a placebo, neither the patient nor the physician knows what product they received). This is done to prevent common biases that can affect the results of non-randomized trials such as the drug in question being given only to the most severe (or less severe) patients, administration of additional drugs that could change the outcome, removal of patients that do not “perform well” after treatment, etc.
Clinical trials take a long time, why wait? If it is safe what is there to lose?
Widespread use of ivermectin can (and already has!) lead to misuse. Ivermectin is widely available as a veterinary drug. If there is a perception that ivermectin is beneficial for COVID-19 patients, it is foreseeable that the veterinary formulations will be used at scale and this unsupervised use may lead to overdosing and other harmful practices. The US FDA has issued a warning about using ivermectin veterinary products.
In Peru, more than 5,000 indigenous were injected with veterinary ivermectin by a group with good intentions, were they conscious that they were being injected with a product intended for animal use?
Along these lines, there are also reports of injection with ivermectin-related veterinary products such as doramectin, a molecule never before used in humans with an unknown safety profile.
If indeed adverse events result from this indiscriminate use, the distribution of the drug for proven indications (e.g. river blindness) might be affected as people might refuse to take the human version of the drug because of the effects in those injecting themselves with veterinary products.
Intestinal parasites are widely prevalent in the tropics. We know that intestinal helminths modulate the way our immune system reacts to inflammation and infection. Given that ivermectin is a very good dewormer, we do not know how mass deworming may affect the way the body responds against SARS-CoV-2. Primum non nocere or perhaps primum ivermectinum, secundum non nocere?
Moral hazard. Those receiving ivermectin as treatment or prophylaxis may feel protected and comply less efficiently with proven measures such as face masks and social distancing.
Finally, we have the utmost steem for frontline health workers and do not judge the decisions and desperation of those facing dying or worsening patients. But could the use of ivermectin (which is relatively safe) be a way to offer something and reduce political and public pressure on policy makers and health authorities?
Then why is it in the national guidelines in Peru, Bolivia and several municipalities in Brazil?
Many countries, faced with an exponential increase in the number of cases and deaths, were actively screening the horyzon for emerging preventive measures and treatments. The Caly et al. in vitro report which made emphatic claims given the doses used set the stage for ivermectin but it was quickly followed by what seems to be fraudulent report showing alleged excellent results in a case-control study. That Surgisphere preprint, although later retracted, is still amply quoted as evidence of ivermectin´s efficacy against COVID-19, particularly in LatinAmerica.
Contrary to many places in the world, ivermectin is locally produced in the form of a drops formulation in many countries in latinamerica. This local availability may have played a role in its popularity.
But there is additional efficacy evidence from other studies!
The trials with results currently available are not the gold standard Randomized-controlled (preferably double blind=) trials. They are mostly case-control studies and even studies that compare two completely different drug schemes which can hardly prove the benefit of ivermectin. The pyramid of evidence in clinical medicine (By Akobeng in BMJ) is provided below for reference. One should be careful with isolated reports of “good clinical experience” given the risk of bias mentioned above. Sometimes even ecological data is used to support claims of efficacy or lack of efficacy of ivermectin against COVID-19, but these whole-country datasets can be twisted in ways that reflect better the views of the analyst.
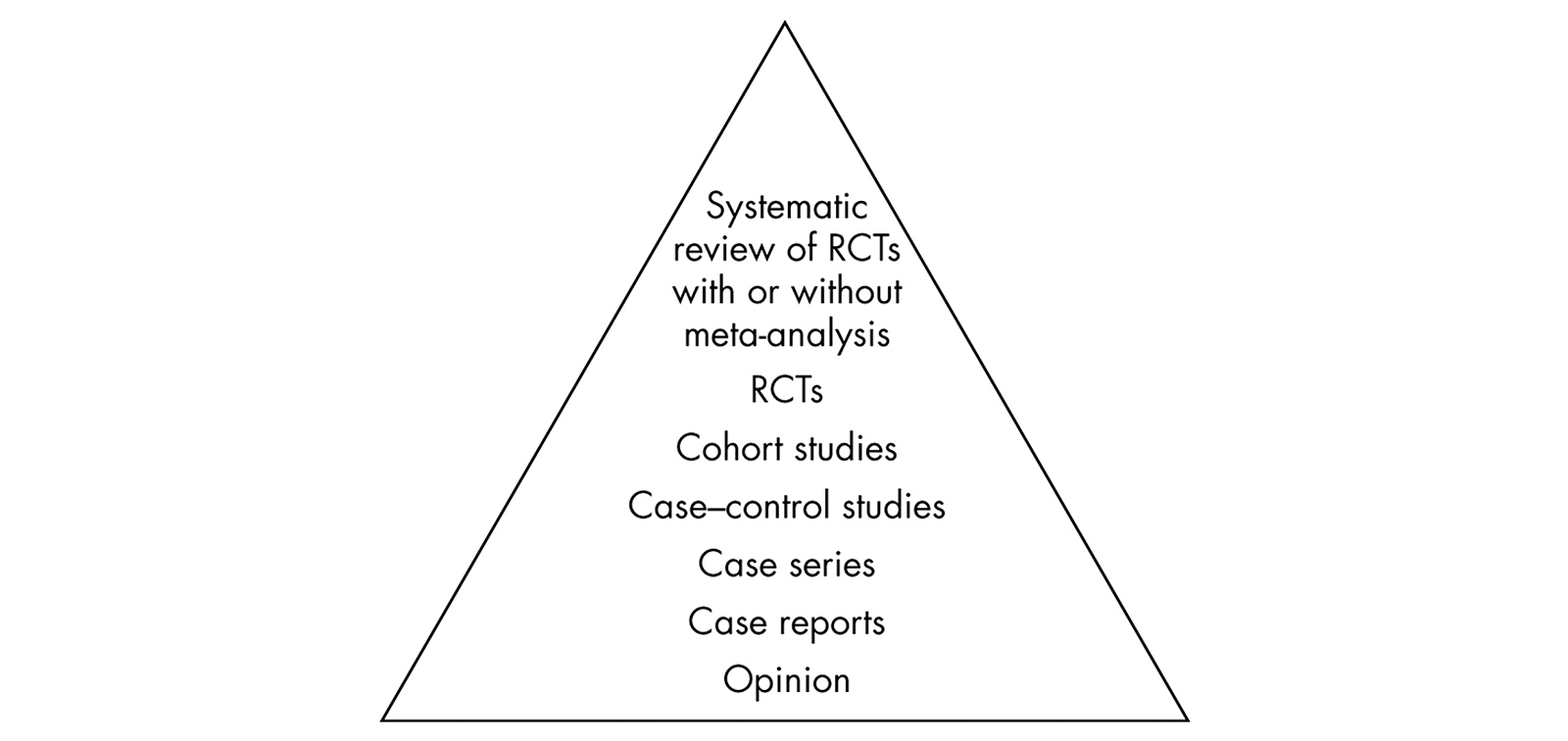
Hierarchy of evidence for questions about the effectiveness of an intervention or treatment. [Source: Akobeng AK. Understanding randomised controlled trials. Archives of Disease in Childhood 2005;90:840-844.]
What clinical trials are ongoing?
According to ClinicalTrials.gov, there are 34 trials using ivermectin in COVID-19 patients, of these 31 are still active (as of 17/august/2020). None of the trials marked as completed have results available in that platform.
Big pharma does not want ivermectin to be used because they want to profit from more expensive drugs!
There are several business models in the pharmaceutical industry. Selling low volumes at high prices is an option for profit. But in the case of COVID-19, the target market is humanity, or about seven billion people that are susceptible to taking this drug now and in the near future. Even with very very very low margins, such high volume would definitely compensate any manufacturer willing to scale up production and distribution.
What has ISGlobal done on this subject?
ISGlobal has partnered with the Clinica Universidad de Navarra to sponsor a clinical trial, SAINT, that could help prove the concept of a biological effect of ivermectin on the replication of SARS-CoV-2. The protocol of this trial is openly available in full for anyone who would like to replicate it. The trial in Navarra has already recruited 20% of its target and the results should be available four weeks after recruiting the last patient. Recruitment has been slower than anticipated because the regulatory approval came during the lockdown that drove cases to levels as low as 0-4 cases per day in the whole of Navarra through June and July.
ISGlobal has partnered with the Clinica Universidad de Navarra to sponsor a clinical trial, SAINT, that could help prove the concept of a biological effect of ivermectin on the replication of SARS-CoV-2
ISGlobal has partnered with the Universidad Cayetano Heredia in Perú to replicate the SAINT trial in Lima.
Several ISGlobal researchers played a key role in unveiling the #LancetGate scandal about hydroxychloroquine and ivermectin.
Additional trials are ongoing and their results will be disseminated in due time.
Updates
1 On December 17, 2020, the answer to question "What about the Importin alpha/beta?" was updated. Due to the emergence of new evidence, the following sentence was removed: "This is very puzzling as SARS-CoV-2 replicates in the cytosol. It does not enter the nucleus for replication. So the amply quoted importin mechanism is unlikely to have a role here." And replaced with this new one: "This may have an effect on COVID-19 through a direct or indirect mechanism".
Related contents
Ivermectina y COVID-19: ¿qué está pasando?
Stay informed on the COVID-19 scientific updates and other global health issues. Click here to sign up for email updates from ISGlobal.


